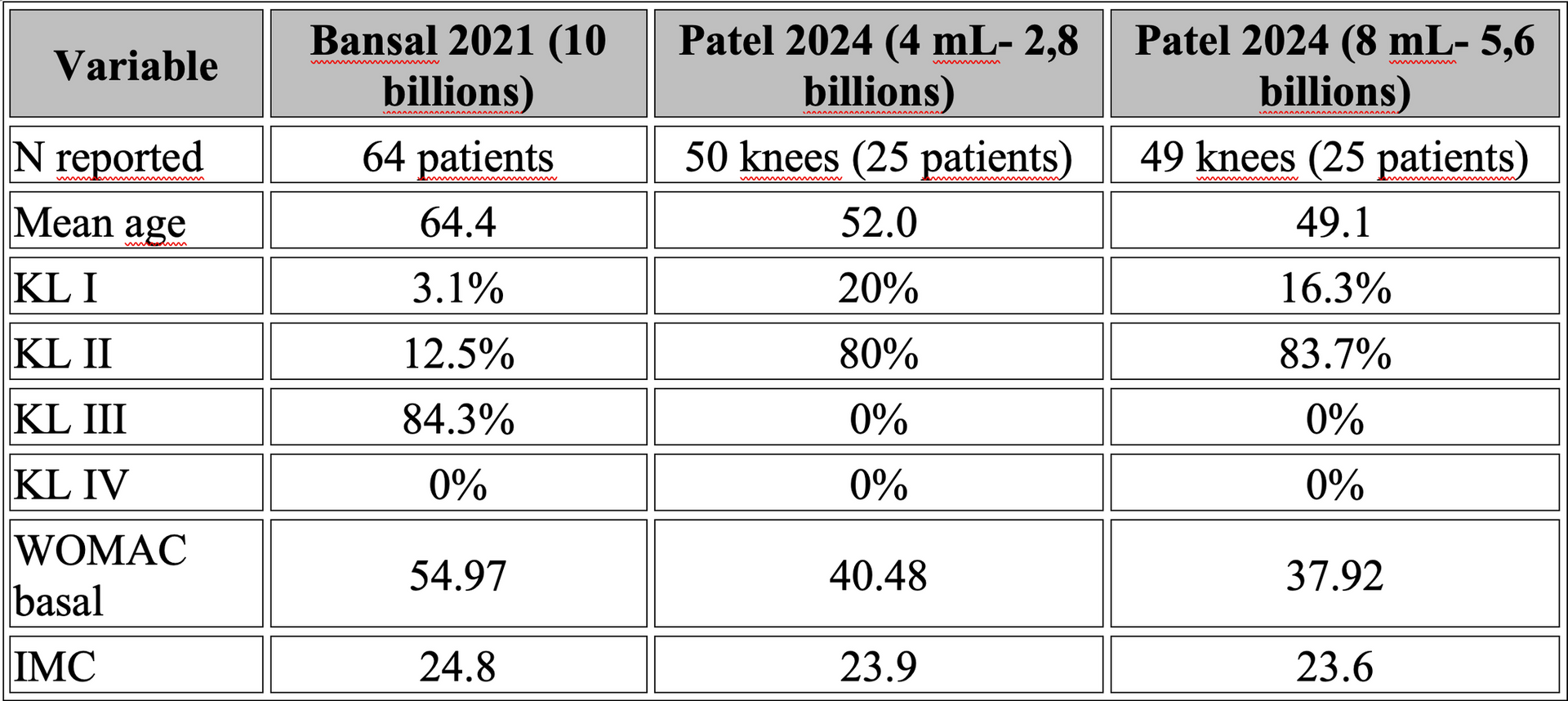
One study treated predominantly KL III patients with substantially worse baseline symptoms, while the other focused on much younger patients with earlier disease stage.
These are not the same clinical phenotype.
This raises an uncomfortable question:
𝗔𝗿𝗲 𝘄𝗲 𝘀𝘂𝗿𝗲 𝘄𝗲 𝗮𝗿𝗲 𝗺𝗲𝗮𝘀𝘂𝗿𝗶𝗻𝗴 𝘁𝗵𝗲 𝗲𝗳𝗳𝗲𝗰𝘁 𝗼𝗳 𝗱𝗼𝘀𝗲... 𝗮𝗻𝗱 𝗻𝗼𝘁 𝘁𝗵𝗲 𝗲𝗳𝗳𝗲𝗰𝘁 𝗼𝗳 𝗽𝗮𝘁𝗶𝗲𝗻𝘁 𝘀𝗲𝗹𝗲𝗰𝘁𝗶𝗼𝗻?
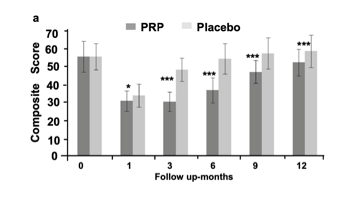
Even more interesting, the study by Bansal and collaborators is often cited as evidence that 10 billion platelets are "critical" for long-term efficacy.
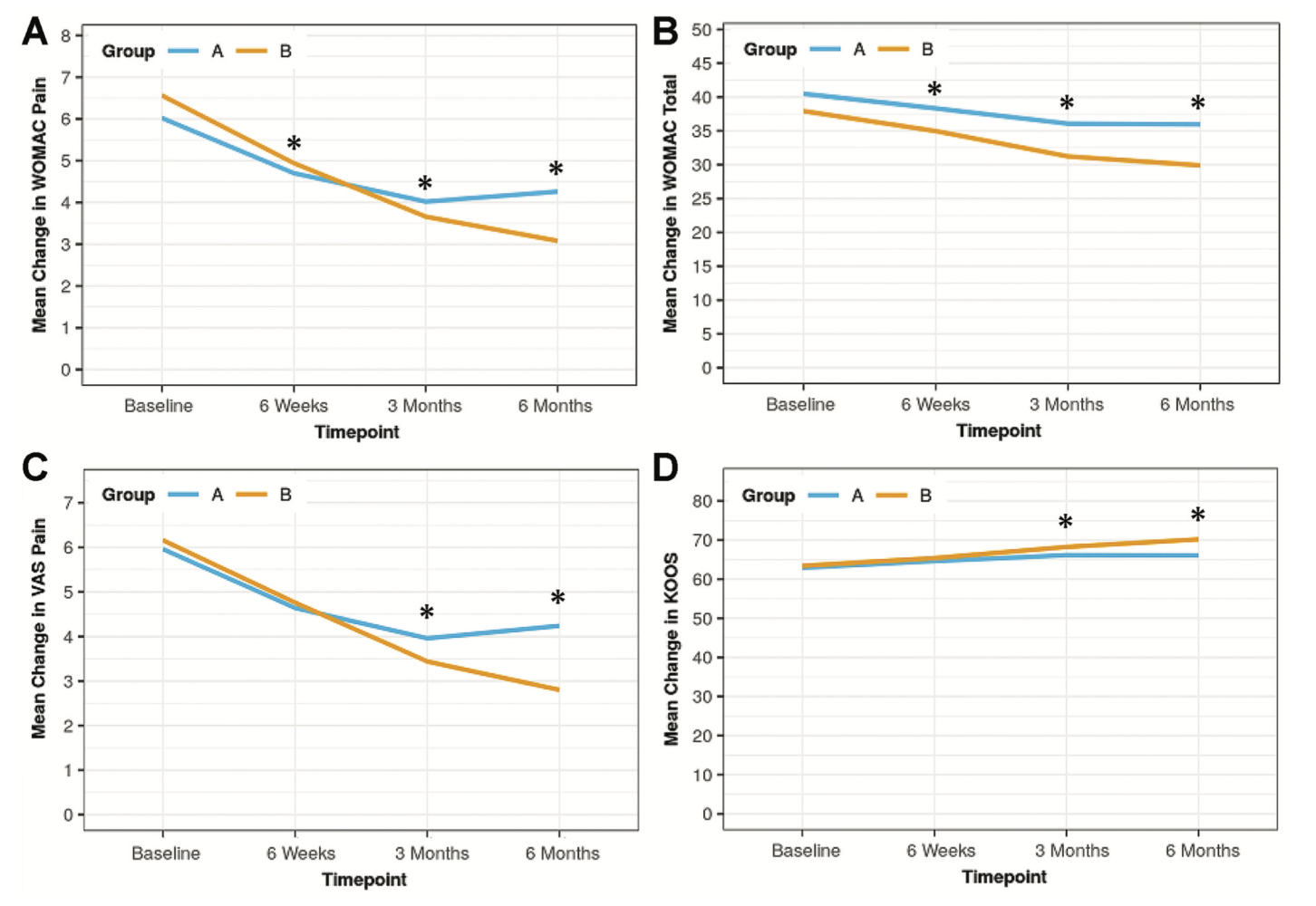
However, when examining the WOMAC and IKDC curves, a different picture emerges.
The clinical response peaks during the first months after injection and progressively declines thereafter.
At 12 months, patients remain “statistically” better than the HA group, but much of the initial improvement has been lost almost completely (compared to baseline). See below.